Current Psychological Distress, Post-traumatic Stress, and Radiation Health Anxiety Remain High for Those Who Have Rebuilt Permanent Homes Following the Fukushima Nuclear Disaster

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
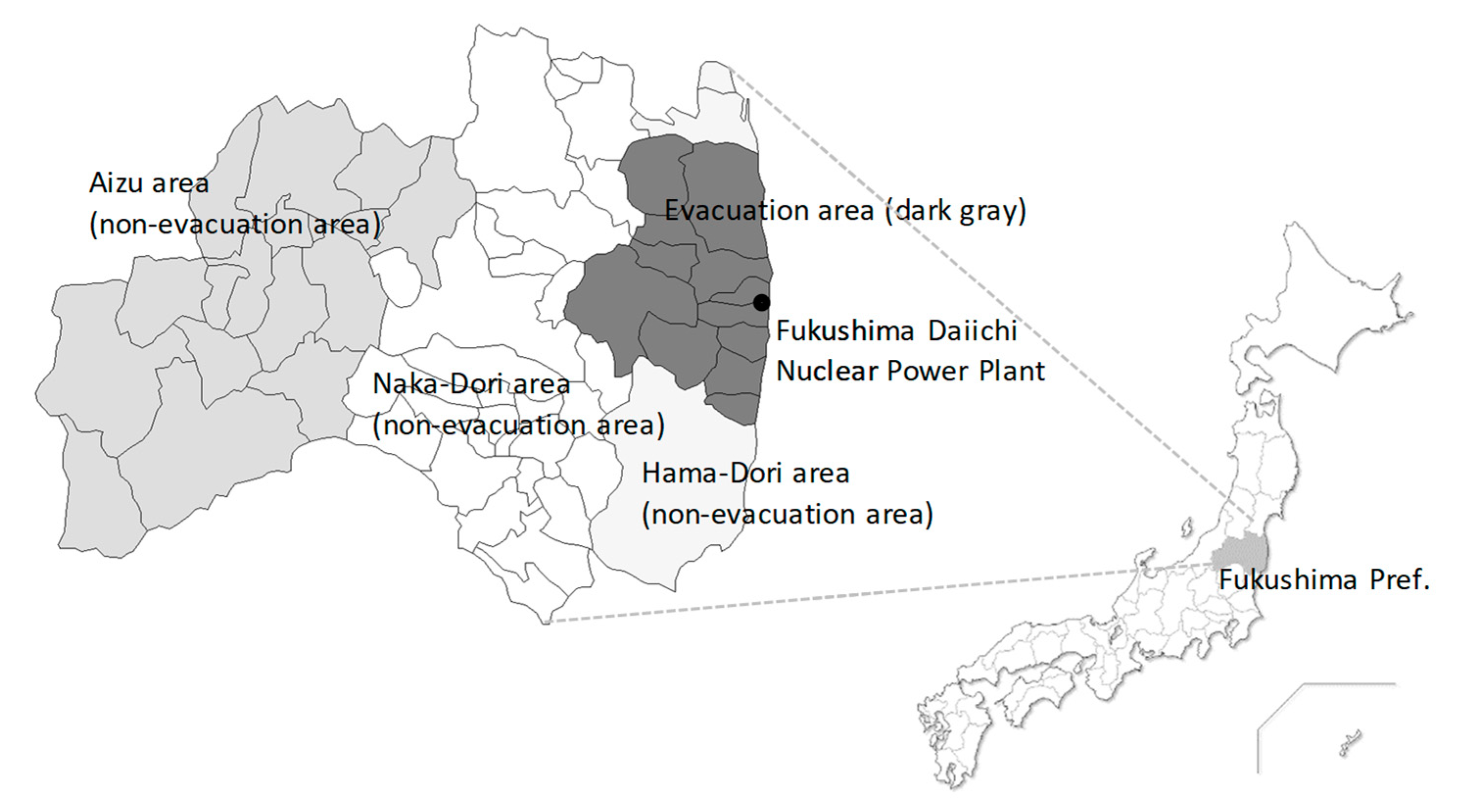
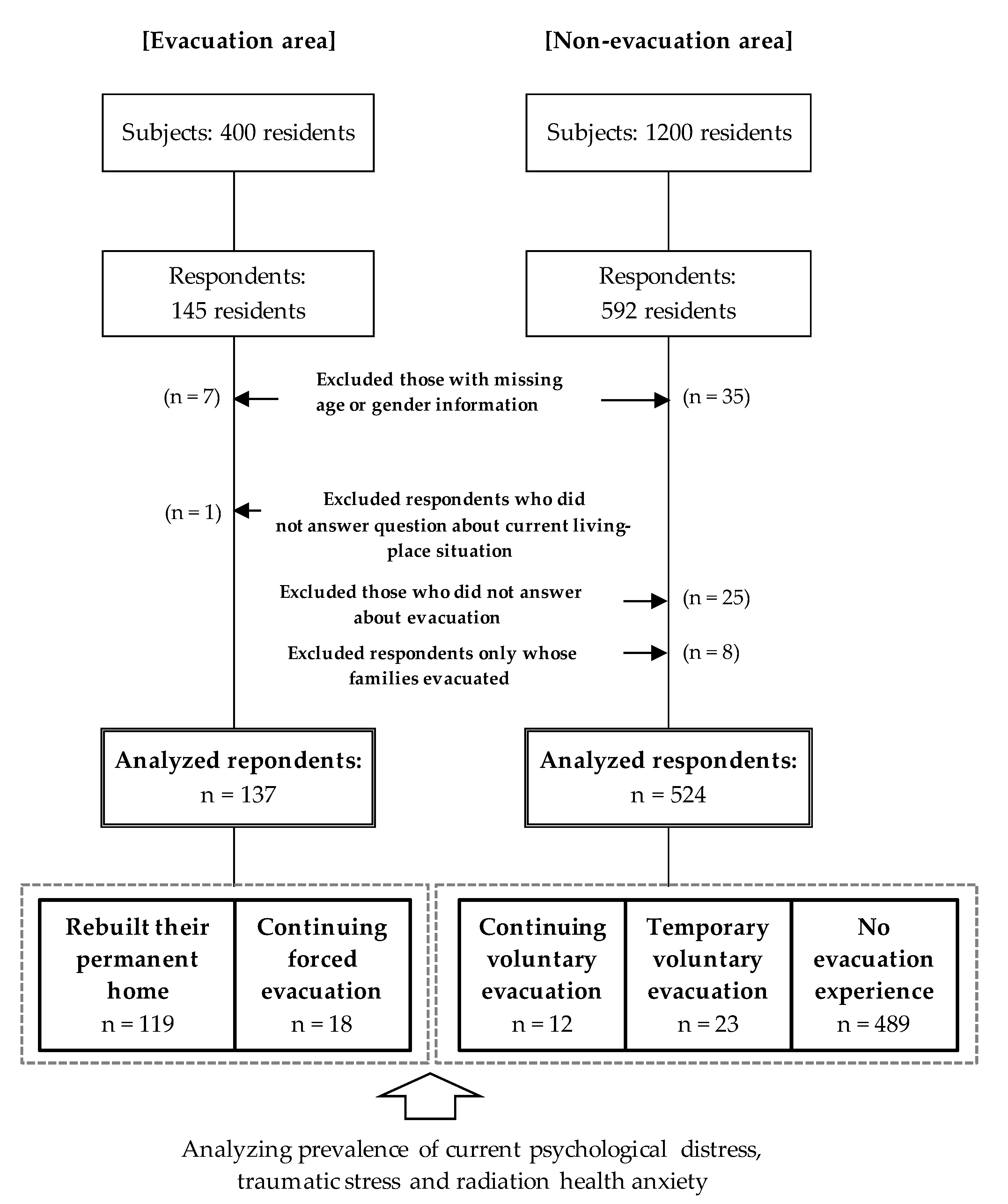
2.1. Participants
2.2. Survey Variables
2.2.1. Current Lifestyle
2.2.2. Psychological Distress
2.2.3. Post-Traumatic Stress
2.2.4. Health Anxiety Due to Radiation Exposure and Media Utilization about Radiation
2.2.5. Classification for Forced or Voluntary Evacuation for Past and Ongoing Experiences
2.3. Statistical Analysis
3. Results
3.1. Participants
3.2. Respondent Characteristics
3.3. Current Lifestyle and Strong Radiation Health Anxiety and Media Utilization about Radiation
3.4. Psychological Distress Current Lifestyle Health Anxiety Due to Radiation Exposure
3.5. Comparison between Those Who Have Rebuilt Their Permanent Home and Those with No Evacuation Experience
4. Discussion
4.1. Previous and Current Statuses of Psychological Distress, Post-Traumatic Stress, and Radiation Health Anxiety among Forced Evacuees
4.2. Lifestyle and Psychological Distress of Evacuees Who Have Rebuilt Their Permanent Home
4.3. Post-Traumatic Stress and Radiation Health Anxiety of Evacuees Who Have Rebuilt Their Permanent Home
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fukushima Revitalization Station, Fukushima Prefectural Office. Damage Caused by the 2011-Earthquake and Tsunami. 2019. Available online: http://www.pref.fukushima.lg.jp/site/portal-english/en03-01.html (accessed on 7 December 2020).
- Ohira, T.; Shimura, H.; Hayashi, F.; Nagao, M.; Yasumura, S.; Takahashi, H.; Suzuki, S.; Matsuzuka, T.; Suzuki, S.; Iwadate, M.; et al. Absorbed radiation doses in the thyroid as estimated by UNSCEAR and subsequent risk of childhood thyroid cancer following the Great East Japan Earthquake. J. Radiat. Res. 2020, 61, 243–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yabe, H.; Suzuki, Y.; Mashiko, H.; Nakayama, Y.; Hisata, M.; Niwa, S.; Yasumura, S.; Yamashita, S.; Kamiya, K.; Abe, M.; et al. Psychological distress after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant accident: Results of a mental health and lifestyle survey through the Fukushima Health Management Survey in FY2011 and FY2012. Fukushima J. Med. Sci. 2014, 60, 57–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shigemura, J.; Tanigawa, T.; Nishi, D.; Matsuoka, Y.; Nomura, S.; Yoshino, A. Associations between disaster exposures, peritraumatic distress, and posttraumatic stress responses in Fukushima nuclear plant workers following the 2011 nuclear accident: The Fukushima NEWS Project study. PLoS ONE 2014, 19, e87516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oe, M.; Fujii, S.; Maeda, M.; Nagai, M.; Harigane, M.; Miura, I.; Yabe, H.; Ohira, T.; Takahashi, H.; Suzuki, Y.; et al. Three-year trend survey of psychological distress, post-traumatic stress, and problem drinking among residents in the evacuation zone after the Fukushima Daiichi Nuclear Power Plant accident [The Fukushima Health Management Survey]. Psychiatry Clin. Neurosci. 2016, 70, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, R.; Takahashi, M.; Sun, S.; Ben-Ezra, M. Psychological distress among tsunami refugees from the Great East Japan earthquake. BJPsych Open 2015, 1, 92–97. [Google Scholar] [PubMed]
- Suzuki, Y.; Yabe, H.; Yasumura, S.; Ohira, T.; Niwa, S.; Ohtsuru, A.; Mashiko, H.; Maeda, M.; Abe, M.; Mental Health Group of the Fukushima Health Management Survey. Psychological distress and the perception of radiation risks: The Fukushima health management survey. Bull. World Health Organ. 2015, 93, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Takebayashi, Y.; Yasumura, S.; Murakami, M.; Harigane, M.; Yabe, H.; Ohira, T.; Ohtsuru, A.; Nakajima, S.; Maeda, M. Changes in risk perception of the health effects of radiation and mental health status: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2018, 15, 1219. [Google Scholar] [CrossRef] [Green Version]
- Maeda, M.; Oe, M. Mental health consequences and social issues after the Fukushima Disaster. Asia Pac. J. Public Health 2017, 29, 36S–46S. [Google Scholar] [CrossRef]
- Orui, M.; Suzuki, Y.; Maeda, M.; Yasumura, S. Suicide rates in evacuation areas after the Fukushima Daiichi Nuclear Disaster: A 5-Year follow-up study in Fukushima Prefecture. Crisis 2018, 39, 353–363. [Google Scholar] [CrossRef]
- Ohto, H.; Yasumura, S.; Maeda, M.; Kainuma, H.; Fujimori, K.; Nollet, K.E. From devastation to recovery and revival in the aftermath of Fukushima’s Nuclear Power Plants Accident. Asia Pac. J. Public Health 2017, 29, 10S–17S. [Google Scholar] [CrossRef] [Green Version]
- Sato, A.; Lyamzina, Y. Diversity of concerns in recovery after a Nuclear Accident: A perspective from Fukushima. Int. J. Environ. Res. Public Health 2018, 15, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orui, M.; Nakajima, S.; Takebayashi, Y.; Ito, A.; Momoi, M.; Maeda, M.; Yasumura, S.; Ohto, H. Mental health recovery of evacuees and residents from the Fukushima Daiichi Nuclear Power Plant accident after seven years—Contribution of social network and a desirable lifestyle. Int. J. Environ. Res. Public Health 2018, 15, 2381. [Google Scholar] [CrossRef] [Green Version]
- Murakami, M.; Takebayashi, Y.; Tsubokura, M. Lower psychological distress levels among returnees compared with evacuees after the Fukushima Nuclear Accident. Tohoku J. Exp. Med. 2019, 247, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueda, Y.; Yabe, H.; Maeda, M.; Ohira, T.; Fujii, S.; Niwa, S.; Ohtsuru, A.; Mashiko, H.; Harigane, M.; Yasumura, S.; et al. Drinking behavior and mental illness among evacuees in Fukushima following the Great East Japan Earthquake: The Fukushima Health Management Survey. Alcohol. Clin. Exp. Res. 2016, 40, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Orui, M.; Ueda, Y.; Suzuki, Y.; Maeda, M.; Ohira, T.; Yabe, H.; Yasumura, S. The Relationship between starting to drink and psychological distress, sleep disturbance after the Great East Japan Earthquake and Nuclear Disaster: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2017, 14, 1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orui, M.; Suzuki, Y.; Goto, A.; Yasumura, S. Factors associated with maintaining the mental health of employees after the Fukushima Nuclear Disaster: Findings from companies located in the evacuation area. Int. J. Environ. Res. Public Health 2017, 15, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Ohira, T.; Maeda, M.; Nakano, H.; Iwasa, H.; Yasumura, S.; Ohtsuru, A.; Harigane, M.; Suzuki, Y.; Horikoshi, N.; et al. The association between self-reported sleep dissatisfaction after the Great East Japan Earthquake, and a deteriorated socioeconomic status in the evacuation area: The Fukushima Health Management Survey. Sleep Med. 2020, 68, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Orui, M.; Nakayama, C.; Kuroda, Y.; Moriyama, N.; Iwasa, H.; Horiuchi, T.; Nakayama, T.; Sugita, M.; Yasumura, S. The association between utilization of media information and current health anxiety among the Fukushima Daiichi Nuclear Disaster evacuees. Int. J. Environ. Res. Public Health 2020, 17, 3921. [Google Scholar] [CrossRef]
- Nakayama, C.; Sato, O.; Sugita, M.; Nakayama, T.; Kuroda, Y.; Orui, M.; Iwasa, H.; Yasumura, S.; Rudd, R.E. Lingering health-related anxiety about radiation among Fukushima residents as correlated with media information following the accident at Fukushima Daiichi Nuclear Power Plant. PLoS ONE 2019, 14, e0217285. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. A Basic Direction for Comprehensive Implementation of National Health Promotion. 2012. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000047330.pdf (accessed on 17 October 2020).
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [PubMed]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD Checklist (PCL). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Iwasa, H.; Suzuki, Y.; Shiga, T.; Maeda, M.; Yabe, H.; Yasumura, S.; Mental Health Group of the Fukushima Health Management Survey. Psychometric evaluation of the Japanese version of the posttraumatic stress disorder checklist in community dwellers following the Fukushima Daiichi Nuclear Power Plant Incident: The Fukushima Health Management Survey. SAGE Open 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, Y.; Yabe, H.; Horikoshi, N.; Yasumura, S.; Kawakami, N.; Ohtsuru, A.; Mashiko, H.; Maeda, M.; Mental Health Group of the Fukushima Health Management Survey. Diagnostic accuracy of Japanese posttraumatic stress measures after a complex disaster: The Fukushima Health Management Survey. Asia Pac. Psychiatry 2017, 9, e12248. [Google Scholar] [CrossRef] [Green Version]
- Hirschel, M.J.; Schulenberg, S.E. On the viability of PTSD Checklist (PCL) short form use: Analyses from Mississippi Gulf Coast Hurricane Katrina survivors. Psychol. Assess. 2010, 2, 460–464. [Google Scholar] [CrossRef]
- Price, M.; Szafranski, D.D.; Stolk-Cooke, K.; Gros, D.F. Investigation of abbreviated 4 and 8 item versions of the PTSD Checklist 5. Psychiatry Res. 2016, 239, 124–130. [Google Scholar] [CrossRef]
- National Reconstruction Agency, Japan. Intentions Survey among Residents in Nuclear-Affected Municipalities. 2019. Available online: https://www.reconstruction.go.jp/topics/main-cat1/sub-cat1-4/ikoucyousa/ (accessed on 22 October 2020). (In Japanese).
- Orui, M. Re-increased male suicide rates in the recovery phase following the Great East Japan Earthquake. Crisis 2020, 41, 422–428. [Google Scholar] [CrossRef]
- Orui, M.; Harada, S.; Saeki, S.; Sato, K.; Kozakai, Y.; Hayashi, M. Trend in the suicide rate following the Great East Japan Earthquake: An eight-year follow-up study in Miyagi Prefecture. Psychiatr. Neurol. Jpn. 2020, 122, 573–584. (In Japanese) [Google Scholar]
- Fukasawa, M.; Kawakami, N.; Umeda, M.; Miyamoto, K.; Akiyama, T.; Horikoshi, N.; Yasumura, S.; Yabe, H.; Bromet, E.J. Environmental radiation level, radiation anxiety, and psychological distress of non-evacuee residents in Fukushima five years after the Great East Japan Earthquake: Multilevel analyses. SSM Popul. Health 2017, 3, 740–748. [Google Scholar] [CrossRef]
- Fukasawa, M.; Kawakami, N.; Umeda, M.; Akiyama, T.; Horikoshi, N.; Yasumura, S.; Yabe, H.; Suzuki, Y.; Bromet, E.J. Longitudinal associations of radiation risk perceptions and mental health among non-evacuee residents of Fukushima prefecture seven years after the nuclear power plant disaster. SSM Popul. Health 2019, 10, 100523. [Google Scholar] [CrossRef] [PubMed]
- The Ministry of Economy, Trade and Industry, Japan. Research Project on Measures against Reputational Damage in Fukushima Prefecture. 2018. Available online: https://www.meti.go.jp/meti_lib/report/H29FY/000636.pdf (accessed on 4 November 2020).
- Horikoshi, N.; Iwasa, H.; Yasumura, S.; Maeda, M. The characteristics of non-respondents and respondents of a mental health survey among evacuees in a disaster: The Fukushima Health Management Survey. Fukushima J. Med. Sci. 2017, 63, 152–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orita, M.; Taira, Y.; Matsunaga, H.; Maeda, M.; Takamura, N. Quality of life and intention to return among former residents of Tomioka Town, Fukushima Prefecture 9 years after the Fukushima Daiichi Nuclear Accident. Int. J. Environ. Res. Public Health 2020, 17, 6625. [Google Scholar] [CrossRef] [PubMed]
- Orui, M.; Kuroda, Y.; Yasumura, S. Suicide rates and mental health measures after the lifting of the evacuation orders following the Fukushima Daiichi Nuclear Power Plant accident: A practical report developed in collaboration with the local municipality. Nihon Koshu Eisei Zasshi 2019, 66, 407–416. (In Japanese) [Google Scholar] [CrossRef]
- Orui, M.; Fukasawa, M.; Horikoshi, N.; Suzuki, Y.; Kawakami, N. Development and evaluation of a gatekeeper training program regarding anxiety about radiation health effects following a nuclear power plant accident: A single-arm intervention pilot trial. Int. J. Environ. Res. Public Health 2020, 17, 4594. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evacuation Experience (+) | Evacuation Experience (−) (n = 489) | |||||
|---|---|---|---|---|---|---|
| Forced Evacuation | Voluntary Evacuation | |||||
| Rebuild Permanent Home | Continuing Forced Evacuation | Continuing Voluntary Evacuation | Temporary Voluntary Evacuation | |||
| (n = 119) | (n = 18) | (n = 20) | (n = 23) | |||
| Age | 20–39 (%) | 13 (10.9%) | 0 (0.0%) | 4 (20.0%) | 3 (13.0%) | 72 (14.7%) |
| 40–59 (%) | 25 (21.0%) | 4 (22.2%) | 5 (25.0%) | 11 (47.8%) | 148 (30.3%) | |
| 60–80 (%) | 81 (68.1%) | 14 (77.8%) | 11 (55.0%) | 9 (39.1%) | 269 (55.0%) | |
| Gender | Male (%) | 66 (55.5%) | 9 (50.0%) | 10 (50.0%) | 9 (39.1%) | 227 (46.4%) |
| Living area | Evacuation area (%) | 119 (100.0%) | 18 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Hama-Dori (%) | 0 (0.0%) | 0 (0.0%) | 9 (45.0%) | 16 (69.6%) | 139 (28.4%) | |
| Naka-Dori (%) | 0 (0.0%) | 0 (0.0%) | 10 (50.0%) | 7 (30.4%) | 174 (35.6%) | |
| Aizu (%) | 0 (0.0%) | 0 (0.0%) | 1 (5.0%) | 0 (0.0%) | 176 (36.0%) | |
| Evacuation Experience (+) | Evacuation Experience (−) | p-Value (χ2 Test) | |||||
|---|---|---|---|---|---|---|---|
| Forced Evacuation | Voluntary Evacuation | ||||||
| Rebuild Permanent Home | Continuing Forced Evacuation | Continuing Voluntary Evacuation | Temporary Voluntary Evacuation | ||||
| (n = 119) | (n = 18) | (n = 12) | (n = 23) | (n = 489) | |||
| Current lifestyle | |||||||
| Sleep condition | Dissatisfied (%) | 24 (20.5%) | 1 (5.6%) | 1 (10.0%) | 3 (13.0%) | 64 (13.1%) | p = 0.233 (χ2 = 5.58) |
| Drinking behavior | Above proper drinking level (%) | 42 (35.6%) | 6 (33.3%) | 2 (20.0%) | 5 (21.7%) | 135 (27.7%) | p = 0.402 (χ2 = 4.03) |
| Health anxiety due to radiation exposure | |||||||
| Strong radiation health anxiety | Very and extremely high (%) | 15 (12.9%) | 2 (11.8%) | 1 (9.1%) | 3 (13.0%) | 26 (5.4%) | p = 0.044 (χ2 = 9.81) |
| Media utilization about radiation | Local media (%) | 81 (68.1%) | 15 (83.3%) | 7 (58.3%) | 16 (70.0%) | 384 (78.5%) | p = 0.062 (χ2 = 8.95) |
| National media (%) | 28 (23.5%) | 9 (50.0%) | 4 (33.3%) | 8 (35.0%) | 214 (43.8%) | p = 0.001 (χ2 = 17.6) | |
| Public broadcasting, (NHK) (%) | 68 (57.1%) | 10 (55.6%) | 4 (33.3%) | 11 (47.8%) | 266 (54.4%) | p = 0.572 (χ2 = 2.92) | |
| Any Internet media (%) | 28 (23.5%) | 3 (16.7%) | 5 (41.7%) | 10 (43.5%) | 151 (30.9%) | p = 0.171 (χ2 = 6.40) | |
| Public relations from local government (%) | 46 (38.7%) | 6 (33.3%) | 4 (33.3%) | 7 (30.4%) | 138 (28.3%) | p = 0.229 (χ2 = 5.63) | |
| Evacuation Experience (+) | Evacuation Experience (−) | p-Value (ANCOVA) * | |||||
|---|---|---|---|---|---|---|---|
| Forced Evacuation | Voluntary Evacuation | ||||||
| Rebuilt Permanent Home | Continuing Forced Evacuation | Continuing Voluntary Evacuation | Temporary Voluntary Evacuation | ||||
| (n = 119) | (n =18) | (n = 12) | (n = 23) | (n = 489) | |||
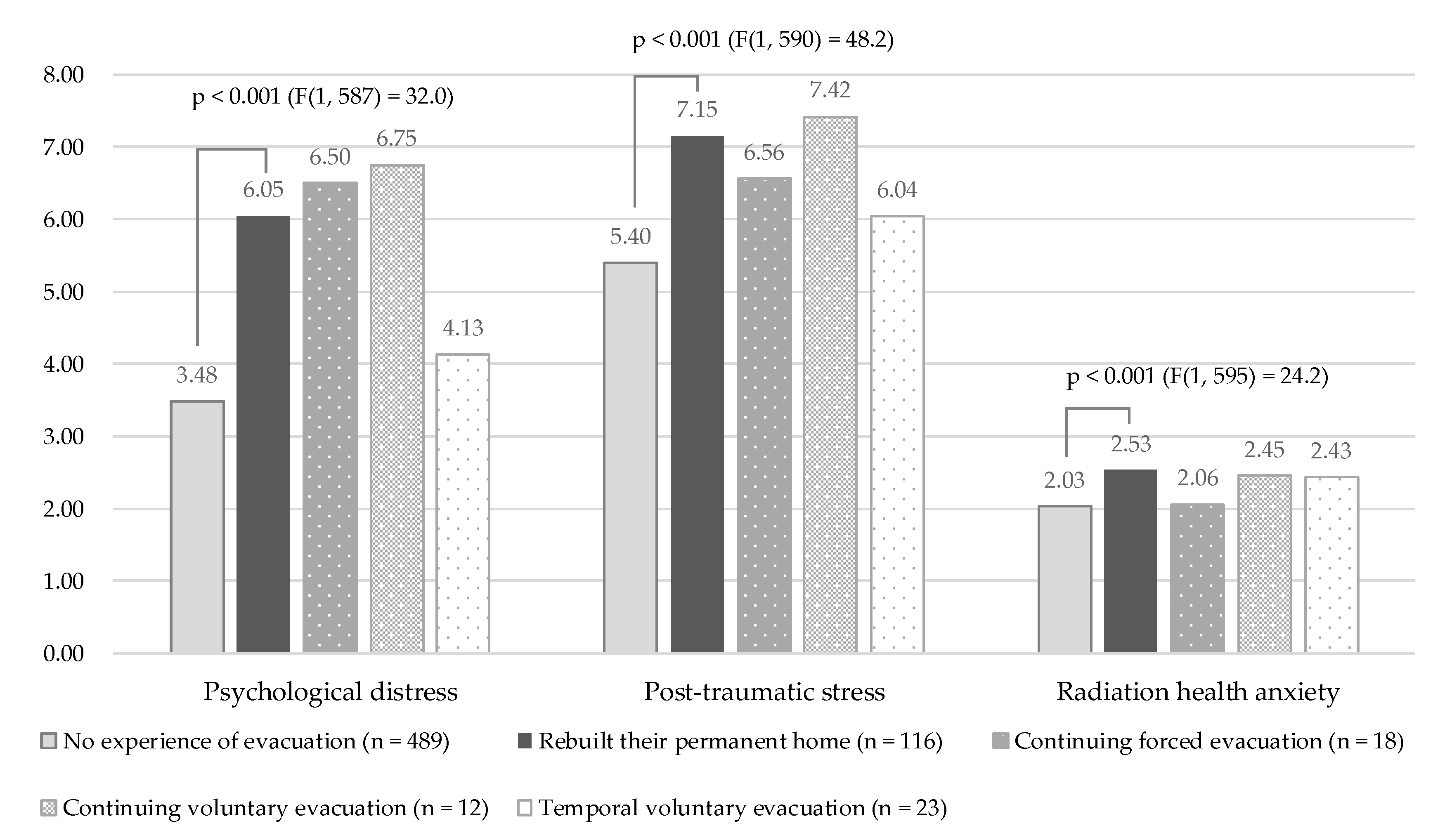
| Psychological distress (K6) | Mean (SD) | 6.05 (5.50) | 6.50 (5.90) | 6.75 (5.55) | 4.13 (3.70) | 3.48 (4.11) | p < 0.001 (F(4, 64) = 10.29) |
| Post-traumatic stress (four-item PCL) | Mean (SD) | 7.15 (3.26) | 6.56 (2.36) | 7.42 (3.75) | 6.04 (3.84) | 5.40 (2.08) | p < 0.001 (F(4, 64) = 13.02) |
| Radiation health anxiety | Mean (SD) | 2.53 (1.07) | 2.06 (1.20) | 2.45 (1.04) | 2.43 (1.12) | 2.03 (1.00) | p < 0.001 (F(4, 64) = 6.67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orui, M.; Nakayama, C.; Moriyama, N.; Tsubokura, M.; Watanabe, K.; Nakayama, T.; Sugita, M.; Yasumura, S. Current Psychological Distress, Post-traumatic Stress, and Radiation Health Anxiety Remain High for Those Who Have Rebuilt Permanent Homes Following the Fukushima Nuclear Disaster. Int. J. Environ. Res. Public Health 2020, 17, 9532. https://doi.org/10.3390/ijerph17249532
Orui M, Nakayama C, Moriyama N, Tsubokura M, Watanabe K, Nakayama T, Sugita M, Yasumura S. Current Psychological Distress, Post-traumatic Stress, and Radiation Health Anxiety Remain High for Those Who Have Rebuilt Permanent Homes Following the Fukushima Nuclear Disaster. International Journal of Environmental Research and Public Health. 2020; 17(24):9532. https://doi.org/10.3390/ijerph17249532
Chicago/Turabian StyleOrui, Masatsugu, Chihiro Nakayama, Nobuaki Moriyama, Masaharu Tsubokura, Kiyotaka Watanabe, Takeo Nakayama, Minoru Sugita, and Seiji Yasumura. 2020. "Current Psychological Distress, Post-traumatic Stress, and Radiation Health Anxiety Remain High for Those Who Have Rebuilt Permanent Homes Following the Fukushima Nuclear Disaster" International Journal of Environmental Research and Public Health 17, no. 24: 9532. https://doi.org/10.3390/ijerph17249532